Ebola Update DRC & Uganda (June 2026)
The current Ebola outbreak in the Democratic Republic of Congo (DRC) and Uganda is the fastest-growing outbreak recorded in history. On Friday, June 26th, the United States Centers for Disease Control and Prevention (CDC) increased the Ebola response level to the highest possible, while the risk of a global threat remains low. This outbreak has been unique because of the strain, complexities in the region, and lack of resources. Below is a brief timeline of the outbreak with cases, locations, risk assessment, travel restrictions, and some complexities to consider.
TIMELINE & CASES
The outbreak was recognized on May 5, 2026, when a cluster was tested in DRC. A retrospective assessment was conducted from April 15-May 13 and identified 246 cases and 65 deaths. That means that the disease had been spreading for over three weeks without anyone knowing. By June 22nd, over 1,000 confirmed cases had been reported. As of June 27th, nearly 1,300 cases have been confirmed with 362 deaths. The case fatality rate (percentage of deaths of those infected) has ranged from 25.8% to 54.7% (28.3% average). That means that in some provinces, one in four people with the disease will likely die, and in other provinces, one in every two people infected will likely die. Read the section on complexities for more information on disease transmission and confirmed/suspected cases.
LOCATIONS
The origin of the outbreak was in the Ituri province located in the north eastern region of DRC, bordering western Uganda. Two other DRC provinces on the eastern side of DRC also have reported cases, North Kivu and South Kivu, bordering Rwanda and Burundi. Uganda has reported 20 cases and two deaths so far (Kampala and Wakiso), while Rwanda and Burundi have not seen any transmission. Read more below about complexities with testing facilities.
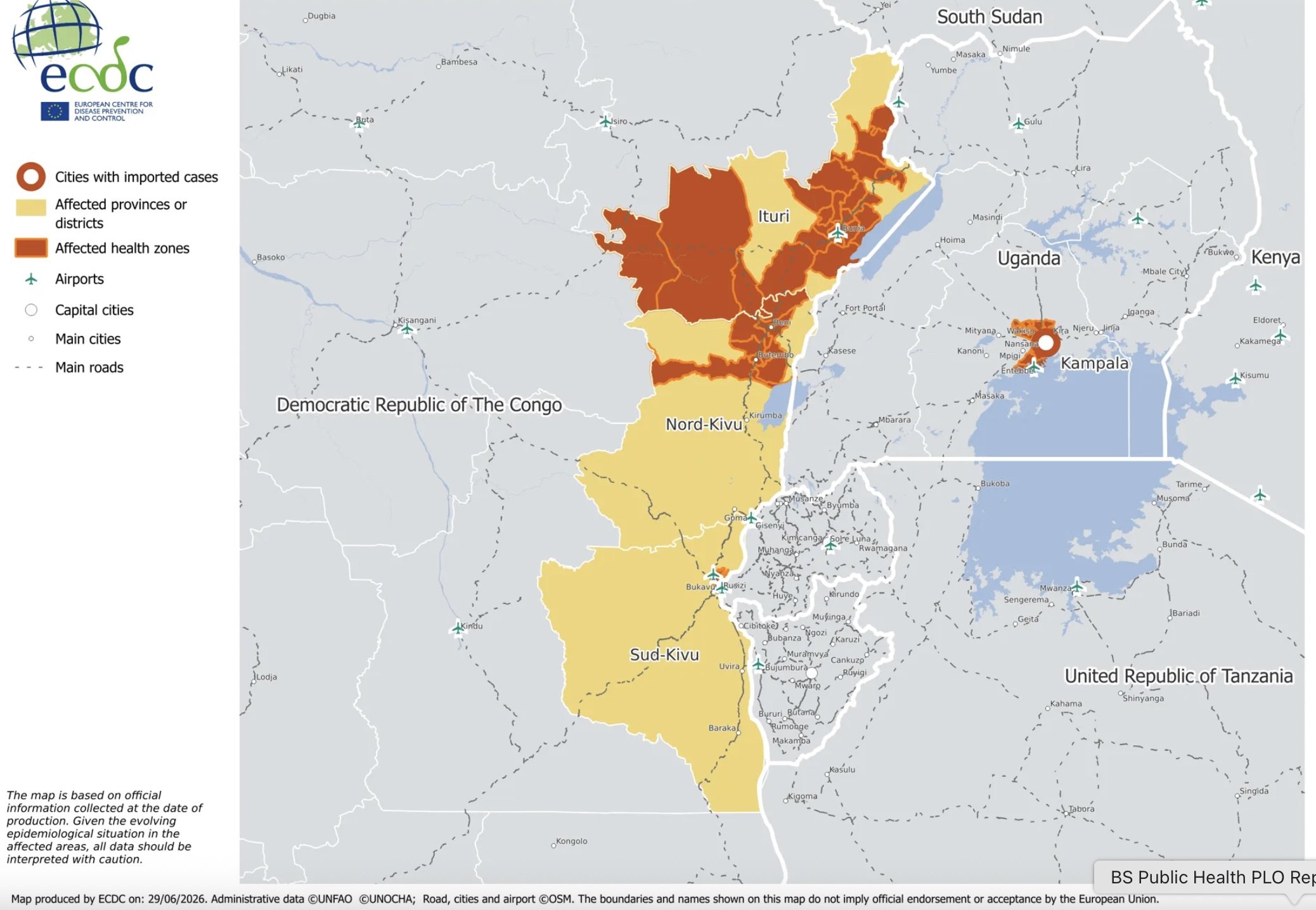
Figure 1. European Centre for Disease Prevention and Control map of DRC/Uganda Ebola outbreak June, 2026.
RAPID RISK ASSESSMENT
The World Health Organization (WHO) released a Rapid Risk Assessment in June. The methodology for assigning risk levels can be found in the resources at the bottom of the page. The levels are ranked low, moderate, high, and very high.
The risk for human health is currently ranked in DRC as very high and in Uganda as high.
The risk for insufficient control capabilities with available resources is ranked in DRC as very high and in Uganda as high.
Testing capacity was also assessed.
DRC has scaled up testing. The Ministry of Health has been implementing a decentralized testing method to expand access to testing and reach remote areas. The country is working on securing a new rapid test kit (RADIONE), which can deliver test results in just 65 minutes. Rapid testing is vital for responses to reduce contacts and minimize the spread of disease.
Uganda has not scaled testing and has not reported anything about rapid test kits. Currently, there are only four testing sites available for the entire country.
TRAVEL RESTRICTIONS
The US has issued the highest alert, Level 4 “Do Not Travel”, for DRC and Uganda. They also placed a ban on travel to the US from DRC, Uganda, and South Sudan with an end date that keeps getting extended (currently set at July 21, 2026). Canada and most European countries have similar alert issues advising residents not to travel to DRC, Uganda, and South Sudan. They require all incoming travelers from those regions to quarantine for 21 days upon arrival.
Currently, there are no flights in or out of Goma and Kavumu in the eastern part of DRC. One of the most popular airlines in Uganda, KLM, has suspended flights through at least July 1st. They will assess current alerts on that date and determine whether to extend the suspension or resume travel.
COMPLEXITIES
Transmission
This outbreak comes with many complexities, unknowns, and questions we should be asking. It is extremely alarming that the outbreak was going on for over three weeks before it was detected. Ebola is a disease that has a 21-day incubation period, meaning a person can be infected for three weeks and not know before symptoms start. Then when symptoms start, it looks like many common illnesses in the region, such as the flu, COVID, or even malaria. It begins with flu-like symptoms and progresses to gastrointestinal issues, followed by internal/external bleeding and organ failure in severe cases. One of the challenges with this disease is that it spreads through bodily fluids (blood, sweat, mucous, saliva, breastmilk, amniotic fluid, semen). This also includes items such as clothes, bedding, needles, and medical equipment that have come in contact with those fluids from an infected person.
Women and Healthcare Workers. The disease has been known as the disease of compassion because it is often transmitted from an infected person to a loved one caring for them through their painful symptoms. Traditionally, women tend to be infected at higher rates of Ebola, not because of biological reasons, but because they are often the caregivers for sick family members. Cases are often seen among healthcare workers as well, especially when they care for an infected person before testing has taken place or when personal protective equipment (PPE) is not available.
Other High Risk Populations. It is not only a terrifying disease that kills anywhere from 30-90% of those infected, but the risk is higher for some populations. The case fatality rate ranges based on the strain of the disease, access to care, vaccine availability, and the population infected. Pregnant women have a higher case fatality rate for all strains, averaging 86%. An extremely sad statistic relating to that is the fetal case fatality rate. If Ebola is transmitted from mother to child during pregnancy, the fetal case fatality rate is nearly 100%. That rate remained the same whether or not the mother survived. People infected with malaria, a highly prevalent disease in the region, also have a higher risk of death from Ebola. Another group disproportionately impacted with higher case fatality rates from Ebola is people living with HIV. As mentioned above, women (caregivers) and healthcare workers are common populations that are infected first, and I have not seen data on those two populations with pregnancy status, malaria, or HIV diagnosis reports.
Transmission Post-Mortem. Most bacterial and viral diseases die when a person dies (the host). Ebola is unique because it can live in bodily fluids for a week after a person dies! That means a person remains highly contagious as any post-mortem examinations, rituals, and burials take place. Funerals can spark cluster outbreaks if loved ones hug, prepare, or kiss the body of an infected person due to sweat or other bodily fluids being present on the body or clothes. It is easy to remove ourselves from the situation and logically state not to have funerals, but it is unimaginable to picture the human emotion side of those decisions. I cannot fathom a family member dying alone in isolation from a painful disease, and then not being allowed to have a funeral or grieve with cultural rituals. The public health practitioner side of me endorses restrictions to protect others so more funerals do not need to happen, but the maternal side of me can’t imagine the heartbreak and pain those families endure. I wish I had endless funding so I could provide proper PPE to mortuaries and families so they could safely say goodbye to their loved ones and begin the grieving process. When Ebola outbreaks happen, we often talk about restrictions and immediate response, but I do not think we follow through with enough mental health and trauma support after the outbreak has ended.
INFRASTRUCTURE SUPPORT
Ebola is not a new disease to DRC or Uganda. In fact, it is a disease that has been around since 1976, primarily in central and western regions of Africa, and has always had a terrifying case fatality rate. It is a horrific disease that no one should have to suffer and die from, and we have the means to prevent it. The DRC, often burdened by these outbreaks, became a model of outbreak preparedness and mitigation. Over the last ten years, 11 of the 12 outbreaks in the region were contained quickly. Seven of those outbreaks had less than 65 total cases. DRC and Uganda built promising health systems that were equipped to detect disease, follow up with contacts, provide isolation and care. Those systems were fractured in 2025 when the US removed funding from the Agency for International Development. The US cut 88% of funding to maternal-child health and 87% of funding for diseases, emerging outbreaks, and surveillance (the systems that would help contain Ebola faster). Those funds helped provide support for community health workers, epidemiologists, disease surveillance specialists, labs, treatment centers, healthcare workers, and more.
Community health workers are at the heartbeat of global health. They are often community members trained to check on their community, test for disease, assist with medication adherence, monitor quarantine, help with transport/care, and alert hospitals and officials when more assistance is needed. Community health workers were paid through US support and only cost $40 per month, but that funding was cut, and the current outbreak spread for weeks before even being detected! The value of community health workers far exceeds the cost of their employment, especially when the risk of outbreaks or disease transmission is so high.
Typically, Ebola outbreaks are identified quickly, response systems are alerted, and the outbreak gets contained. That is why those seven outbreaks in the last ten years only had a handful of cases. The current outbreak went on for over three weeks before anyone even raised a flag to notice. Historically, when an outbreak is reported, it is usually the first case or two. In this outbreak, the first alert happened when 246 cases and 64 deaths had already been confirmed! This number is astronomical when you think about how all of those cases had likely been cared for by family members and health workers with no idea that they were contagious. One of the first clusters was suspected to be from a funeral, from one of those deaths that spread to people attending that came in contact with the body. Ebola has a spreading rate (R0) of 1.3-5.2 people. That means for every person infected with Ebola, they are likely to spread it to 1-5 other people. Using that calculation, we can estimate that those 246 cases would transmit it to about 320-1,300 other people, especially with the diagnosis unknown. It would have been the community health workers that would have identified those sick patients earlier, contact tracers would have helped contact those at risk, surveillance specialists would have monitored where the clusters were starting, and epidemiologists would have mapped the disease and performed calculations. All of those public health roles were missing when this outbreak started, and now we are trying to catch up with limited resources provided too late.
Public health practitioners commonly use two categories for reporting Ebola, confirmed and suspected/probable. Those terms are used with the number of cases and the number of deaths. These numbers help us track where the disease is, how severe it is, and how to prevent it from spreading further. As of right now, the suspected/probable calculations are completely missing from data reports. Those categories are listed as N/A, which highlights a few concerns. We do not have a grasp on the scope of this outbreak if we are only reporting confirmed cases/deaths; contact tracing isn’t happening at the pace it should, and this could be moving faster than we recognize. Based on the little data we do have, public health scientists created modeling projections published in the Morbidity and Mortality Weekly Report. They predict that if only 20% of infected people are in isolation, we could see over 10,000 cases in the next three months (86% of the modeling scenarios). If 70% of patients are in isolation, we can expect less than 10,000 cases in the next three months (94% simulation projecting). Either way, we need to provide more support so that contact tracing, isolation, and care can happen efficiently.
Regional Complexities
Other complexities exist in the region that would make an outbreak like this challenging, even with support. DRC has been under extreme civil unrest and violence (read more about it in the Canadian travel report in the resource list). There have even been attacks on Ebola treatment centers, causing patients to flee. The widespread violence has caused millions of people to be displaced, making it harder to conduct testing and contact tracing. The Ministry of Health has been working to secure rapid test kits and decentralize testing services to reach those in remote or displaced areas.
Uganda accepts the majority of DRC refugees fleeing violence and seeking asylum. They are a generous country and have welcomed hundreds of thousands of DRC refugees seeking help. In April, 2026, Uganda was seeing upwards of 600 new refugees enter the country daily! The majority of refugees cross from the northeastern part of DRC (where the outbreak originated) into the western part of Uganda. The funding cuts have been felt there as well, with the lack of community health workers and screenings. Current WHO reports state that there are only four Ebola testing sites in all of Uganda! Testing needs to be scaled up given the large influx of refugees when the outbreak was starting, and no one knew about it.
Prevention
Health education is a powerful tool in disease prevention in any disease whether it is Ebola, HIV, malaria, or any other. We need to reinstate funding to the public health systems so that proper testing, isolation, and care can happen. We cannot protect people when we do not know where the disease is spreading (lack of testing). People will not take preventive measures such as handwashing, using PPE, or staying home when sick if they are not aware of what symptoms are or where the disease is present. The Meeting TENTS team created Ebola-specific resources for community health workers, teachers, pastors, and health educators to use. If you are one of our partners or are currently located in Uganda or DRC, please email us to get copies of those free training resources (info.meetingtents@gmail.com). We stand with you and are here to help.

Figure 2. Meeting TENTS Sr. Fellow, Joanna, educating community members and distributing Ebola prevention resources in Ugandan communities.
RESOURCES
DRC Ministry of Health Ebola Report June 27 2026
WHO Rapid Risk Assessment June 2026
US CDC Ebola Situation Report June 26 2026
US CDC Highest Level June 2026
Ebola Updates European CDC June 2026
Attacks on Ebola Treatment Facilities May 2026
Why Are There Attacks on Ebola Facilities May 2026
WHO Rapid Risk Assessment Methodology
Canada Detailed Travel Advisory
Historical Ebola Outbreaks through 2022